What is Cartilage Damage?
The articular surfaces (surfaces that make contact with another skeletal structure as part of a joint) of long bones are covered with hyaline cartilage. Damage to this hyaline cartilage is known as a chondral injury or, if the underlying bone is also fractured, an osteochondral injury.
Articular chondral and osteochondral injuries of the knee are common in people aged under 35 years, but a second peak occurs in patients older than 60 years.
Mechanism of injury
Trauma in the form of a rotational, direct force is the most common cause of injury to the articular cartilage and in most cases the injury it is the weight-bearing regions of articular cartilage on the inside of the knee that are effected.
Articular cartilage has little capacity to repair itself or regenerate. Therefore, cartilage defects repair by forming scar tissue. This scar tissue is deficient collagen and has lower load-bearing capacity. This later surface deterioration may progress to give chronic pain and poor function.
Fig 1: Normal Knee Joint
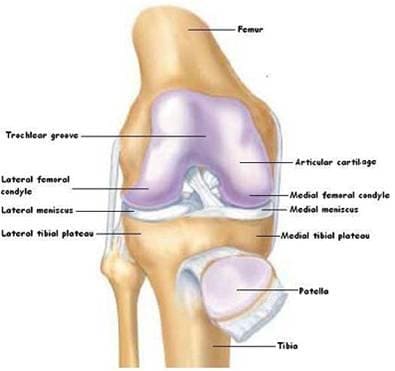
Fig 2: Chondral Defect

Presentation
Articular cartilage has no blood supply and no nerve ending, so pain would not be expected; yet some patients do present with pain. It may be present at rest and is exacerbated by weight-bearing exercises.
The knee may give way if a longstanding injury results in substantial muscle wasting or there is associated ligamentous instability.
Locking is reported if a loose fragment impedes articular movement.
The joint may be swollen.
Tenderness is found on palpation of the joint line, with pain induced by both passive and active movements.
Crepitus is palpable on passive joint movement in a usually stable knee.
Assessment
After a clinical history has been taken, and the joint examined, imaging will be performed to help with the diagnosis. Plain x-rays are used to rule out a more significant fracture, but a MRI scan is needed to accurately assess the joint surface. Sometimes an examination under anaesthetic with an arthroscopy (key-hole surgery to look in the knee with a camera) is needed.
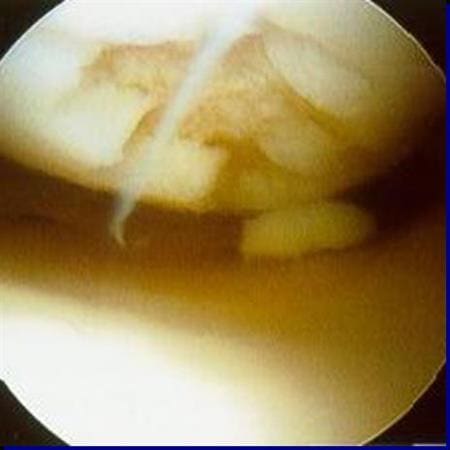
 Arthroscopy picture showing cartilage damage on the knee joint
Arthroscopy picture showing cartilage damage on the knee joint
Management
Lesions may not be diagnosed or may present late because patients will often give a history of an apparently insignificant trauma. Doctors may fail to understand the importance of an effusion in the knee joint, which always indicates joint disease.
Injuries that are new are given time to settle to see if the chondral lesion will become symptomatic or not. If pain fails to resolve after the initial acute phase, and after resting, applying ice, compression bandaging and elevation, surgical intervention is considered.
Surgical
Treatment of larger and symptomatic lesions is surgical and techniques include arthroscopic debridement, marrow-stimulating techniques and cartilage transplantation, either from other parts of the patient’s body that are not needed as much.
Prognosis
Several factors have been associated with improved postoperative recovery.
- Defect size of less than 2 cm.
- Preoperative duration of symptoms of less than 18 months.
- No previous surgical treatment.
- Younger patient age.
- Higher pre-injury level of sports.
- Development of recurrent locking, popping, or effusions after an adequate trial of conservative therapy may suggest the need for surgical intervention.